

We often observe clinical cases in commercial production and wonder whether the conditions reported are the result of immunosuppression caused by a virus or another agent.
We immediately review previous serological evaluations to determine if the immune response has been as expected. That is, whether we detect the expected antibody levels according to the established vaccination program or if there are signs of a field challenge. Precisely because of the importance of quick access to this data, it is necessary to organize it efficiently.
In modern animal production, vaccination, depending on the type of antigen, route of application, and degree of attenuation achieved, consists of creating a mild or subclinical infection to induce a benign form of the disease.
Ideally, this controlled exposure should produce minimal adverse effects that will allow the development of neutralizing antibodies before a field challenge.
It’s important to consider that vaccinations, being stress-inducing practices, can trigger reactions ranging from fever or decreased appetite to death. The live vaccine against Avian Cholera (Pasteurella multocida) is known for producing lethargic birds after its application.
The vaccines most commonly used in poultry farming are inactivated, live, and recombinants:
IMMUNE RESPONSE


During the first weeks of life, lymphocytes produced in the bone marrow are transported through the bloodstream to the primary lymphoid organs (Bursa of Fabricius and thymus).
Here, the maturation of B and T lymphocytes occurs. Once mature, lymphocytes leave the primary lymphoid organs and occupy secondary lymphoid organs: spleen, Harder’s gland, and lymphoid tissue associated with the bronchi and intestines. In the digestive tract, Peyer’s patches, cecal tonsils, and an aggregate of epithelial cells along the intestinal tract are located.
Humoral Immunity. The three most important immunoglobulins produced by bird’s B lymphocytes are named immunoglobulin M (IgM), IgG or IgY, and IgA. The primary immune response is initiated with the development of IgM antibodies, which appear about 4-5 days after exposure and almost completely disappear 10-12 days after the challenge.
IgG is of lower molecular weight than IgM, and its production begins 5 days after exposure with a production peak 2-3 weeks after exposure, followed by a slow decline, representing the antibody that is regularly measured in serological tests.
From a practical point of view, it is very important to wait 2-3 weeks before taking blood samples from birds that have been sick to detect the presence of antibodies resulting from a field exposure.
If blood samples are taken early, the antibodies present will be of the IgM type, and elevated antibodies will not be detected in the serological tests routinely used. IgA is considered a critical element in the development of local immunity in the respiratory and intestinal tracts.
In birds, IgA is transported to the liver for storage in the bile and is present in the serum and mucous membranes (eyes, respiratory system, gastrointestinal system), being considered the most important immunoglobulin for the protection of mucous membranes.
Both IgM and IgG are found in the bloodstream and are detected in Elisa test, agglutination, agar precipitation, complement fixation, and viral neutralization.
Cellular Immunity. T lymphocytes are the main white blood cells associated with cell-mediated immunity. Despite their importance, there are few procedures to quantify this response, which are somewhat difficult to perform and are not routinely used.
Active and Passive Immunity. Both types are used to prevent diseases. Active immunity, obtained by applying live vaccines, is the most commonly used technique in prevention. Passive immunity is frequently used for the control of Gumboro Disease, Avian Encephalomyelitis, and Infectious Anemia virus of chickens.
In the case of Gumboro, newly hatched chicks are very susceptible to the disease if not vaccinated in the first days of life, making early protection critical.
The disadvantage of passive immunity is that it is difficult to determine the optimal time for active immunization in the case of a flock of chicks with different levels of maternal antibodies.
Precisely for this reason, companies that produce newly hatched chicks vaccinate in the incubator or on the farm because they do not rely solely on the presence of maternal antibodies to protect the chicks.
Origin of Maternal Antibodie. During the egg’s passage through the oviduct, maternal antibodies (IgY or IgG) are secreted into the yolk sac by secretory follicles present in the epithelial tissue located on the walls of the chicken’s oviduct.
In the last 5-6 days of embryonic development, a time when the embryo absorbs the yolk, the greatest absorption of IgG occurs in the embryo. IgA has been detected in the egg, but the amount transferred to the chick’s bloodstream is low and usually not detected.
IMMUNE RESPONSE AFTER VACCINATION
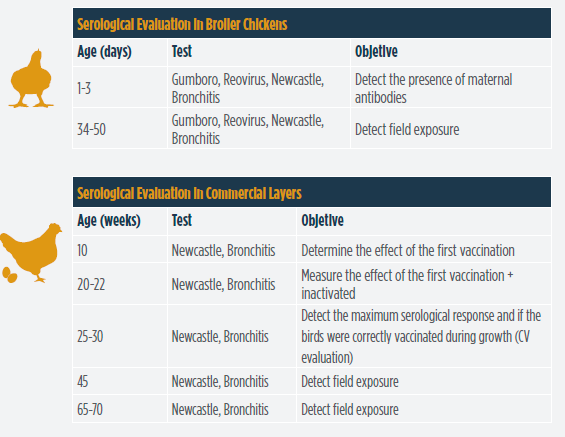
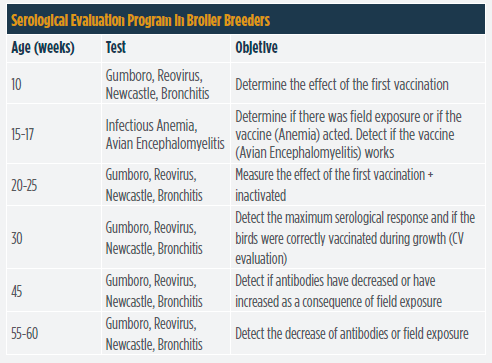
There are several serological tests used to determine the effect of vaccination in birds. The Elisa test is one of the most common and practical. When evaluating the serological response, it is recommended to ideally bleed a minimum of 20 samples per flock following the evaluation program suggested in the tables included in this article.
Unfortunately, for economic reasons, some companies only process 10 samples per house or flock, thus hindering a good evaluation.

In the case of hens, at 20-25 weeks, the uniformity of the titles (coefficient of variation – CV) should be evaluated to determine if the birds have been correctly vaccinated during growth. Normally, the maximum level of antibody production after injecting an inactivated vaccine occurs 4-6 weeks after application.
By evaluating uniformity, it can be determined if the vaccination crews did a good job. Generally, heavy breeders received live vaccines against Newcastle, Bronchitis, and Gumboro, followed by an inactivated vaccine applied at 18-20 weeks.
This program was effective for a time, but it was reported that antibodies began to fall after 40 weeks in the case of Gumboro disease and after 50 weeks for Newcastle and Bronchitis.
The problem with revaccinating birds in production is production drops. So it was decided to apply two inactivated vaccines during the growth stage. With this objective, inactivated vaccines were applied at 10 and 18-20 weeks.
Subsequently, other modifications have been made to the vaccination program, trying to reduce the labor used. With this goal, up to two simultaneous vaccinations have been carried out, in some cases, both vaccines are applied simultaneously at 15 weeks or at 18 weeks.
In conclusion, it is necessary to establish a practical way to organize laboratory results to determine the level of the serological response after vaccinations. The implementation of a vaccination response evaluation plan similar to the one suggested in this article will determine if vaccination has been successful.


Interview Dr. Nivin Nasser

Subscribe now to the poultry technical magazine
AUTHORS

Newcastle Disease: One Hundred Years On, Why Transmission Control Matters More Than Ever
Mustafa Seckin Sandikli
Egg Size Versatility in Nick Chick – Part I
H&N Technical Department
Interview with Khaled Abdel Nasser Awwad
Khaled Abdel Nasser Awwad
When the Supply Chain Breaks: Poultry Prices and the Economics of Maritime Disruption in the Middle East
Dima Chatila
Reovirus Infections in the Broiler Industry
Edgar O. Oviedo Rondón
Egg Condensation in Hatcheries: A Hidden Risk for Embryo Development, Hatchability and Chick Quality
Rasel Ahmed
From Chat to Farm Insight: Bridging the Social Data Gap in Indonesian Broiler Farming
Setiawan Guntarto
Labor Shortage in the Poultry Industry: Potential Solutions
Edgar O. Oviedo Rondón
A Comparison of Soybean Meal from Different Origins in Terms of Nutrient Composition, Amino Acid Profile, and Protein Quality
Güner GÖVENÇ
When Algorithms Start to Control Feed Composition
Henri E. Prasetyo DVM. M.Vsc